

Abstract
BACKGROUND
Lenalidomide (LEN) until progressive disease (PD) is an established treatment (Tx) in newly diagnosed and relapsed and/or refractory multiple myeloma (RRMM); thus, patients (pts) for whom the benefit of LEN has been exhausted are a clinically relevant population. However, LEN-refractory pts have typically been excluded from recent clinical trials investigating triplet regimens after ≤ 3 prior Tx lines. MM-014 (NCT01946477) is an ongoing phase 2 study that was designed to assess the safety and efficacy of pomalidomide (POM)-based Tx regimens in pts with RRMM and first- or second-line LEN Tx failure immediately before study entry. Earlier results from cohort A (POM + low-dose dexamethasone [LoDEX]) and cohort B (POM + LoDEX + daratumumab [DARA]) indicate that POM-based Tx is safe and effective in this setting. Here we report updated results from cohort B.
METHODS
Eligible pts had RRMM, had 1 or 2 prior lines of Tx, received LEN-based Tx as their most recent Tx regimen, and had PD during or after their last line of Tx. Pts received POM 4 mg/day on days 1 through 21 + LoDEX 40 mg/day (20 mg/day if aged > 75 years) on days 1, 8, 15, and 22 and DARA 16 mg/kg intravenously on DEX dosing days of cycles 1 and 2, days 1 and 15 of cycles 3 through 6, then day 1 of cycle 7 and beyond. Each Tx cycle lasted 28 days. Thromboprophylaxis was mandatory. The primary endpoint for cohort B is overall response rate (ORR) by modified International Myeloma Working Group criteria. Secondary endpoints include time to response (TTR), progression-free survival (PFS), time to progression (TTP), and safety.
RESULTS
The intention-to-treat (ITT) population comprised 112 pts (median follow-up, 8.2 mos); data cutoff was April 30, 2018. Median age was 66.5 years, 67.9% of pts were male, and 111 (99.1%) had ECOG PS ≤ 1. A total of 34 pts discontinued Tx: 19 due to PD, 9 due to study withdrawal, 2 due to adverse events (AEs), and 4 due to other reasons. All pts received prior LEN, and 87 (77.7%) received prior bortezomib; 84 pts (75.0%) were refractory to LEN, while 28 (25.0%) relapsed after LEN-based Tx. Median duration of the most recent prior LEN-based Tx was 23.9 mos, with 36 pts (32.1%) receiving LEN 25 mg/day during their last LEN-based Tx.
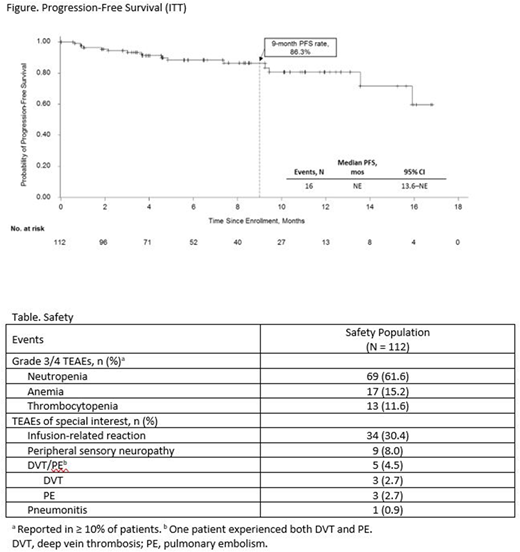
ORR was 77.7%, with 33.9% of pts achieving ≥ very good partial response. Median TTR was 1.0 mo. The clinical benefit rate (≥ minimal response [MR]) was 85.7%. ORR was 80.6% in the efficacy-evaluable population (n = 108; defined as all pts who received ≥ 1 dose of study drug and had ≥ 1 post-baseline response assessment), 75.0% in LEN-refractory pts, and 76.2% in pts with 2 prior lines of Tx (n = 42). The 9-mo PFS rate was 86.3% (range, 76.5%-92.2%); median PFS was not estimable (NE; Figure). The 9-mo TTP rate was 88.1% (range, 78.3%-93.6%); median TTP was NE.
The most common grade 3/4 hematologic treatment-emergent AE (TEAE) in the safety population (n = 112) was neutropenia (61.6%; Table); pneumonia was the most common grade 3/4 nonhematologic TEAE (7.1%). POM dose reductions occurred in 31 pts (27.7%); per protocol, DARA dose reductions were not allowed. POM dose interruptions due to AEs were reported in 69 pts (61.6%) and DARA dose interruptions due to AEs were reported in 82 pts (73.2%). POM and DARA dose interruptions due to neutropenia were reported in 39 (34.8%) and 42 (37.5%) pts, respectively; 25 pts (22.3%) had DARA dose interruptions due to infusion-related reactions. Median durations of POM and DARA Tx were 6.0 mos (range, 0.3-17.7 mos) and 6.6 mos (range, 0.3-18.6 mos), respectively; among those who achieved ≥ MR, pts remained on POM Tx for a median of 7.4 mos (range, 0.9-17.7 mos) and on DARA Tx for a median of 7.5 mos (range, 0.9-18.6 mos).
CONCLUSIONS
LEN-refractory pts with RRMM are in need of effective Tx options. MM-014 is the first prospective clinical trial to investigate a POM-based doublet or triplet regimen immediately after LEN-based Tx failure. In the context of a relatively short follow-up, the 9-mo PFS rate (86.3%) is promising. The ORR (77.7%) was higher than that previously reported with this triplet combination in heavily pre-treated pts with RRMM (≥ 2 prior lines [median, 4]; ORR, 60%), and the rate of grade 3/4 neutropenia in the present study was lower (61.6% vs 77%). These updated results from cohort B continue to demonstrate that POM + LoDEX + DARA is safe and effective following first- or second-line LEN-based Tx failure and further support earlier use of POM-based Tx in pts with RRMM
Siegel:Takeda: Consultancy, Honoraria, Speakers Bureau; Amgen: Consultancy, Honoraria, Speakers Bureau; Novartis: Honoraria, Speakers Bureau; Merck: Consultancy, Honoraria, Speakers Bureau; BMS: Consultancy, Honoraria, Speakers Bureau; Celgene: Consultancy, Honoraria, Research Funding, Speakers Bureau; Karyopharm: Consultancy, Honoraria; Janssen: Consultancy, Honoraria, Speakers Bureau. Schiller:Pharmacyclics: Research Funding; Celator/Jazz Pharmaceuticals: Research Funding. Sebag:Amgen Canada: Membership on an entity's Board of Directors or advisory committees; Takeda Canada: Membership on an entity's Board of Directors or advisory committees; Janssen Inc.: Membership on an entity's Board of Directors or advisory committees; Celgene Canada: Membership on an entity's Board of Directors or advisory committees. Berdeja:Bluebird: Research Funding; Janssen: Research Funding; Sanofi: Research Funding; Takeda: Research Funding; Novartis: Research Funding; Celgene: Research Funding; Bristol-Myers Squibb: Research Funding; Glenmark: Research Funding; Genentech: Research Funding; Amgen: Research Funding; Teva: Research Funding; Poseida Therapeutics, Inc.: Research Funding. Ganguly:Janssen: Consultancy; Seattle Genetics: Speakers Bureau; Amgen: Consultancy; Daiichi Sankyo: Research Funding. Matous:Celgene: Consultancy, Honoraria, Speakers Bureau. Bar:Celgene: Consultancy. Quick:CTI BioPharma: Research Funding. Fonseca:Celgene: Speakers Bureau. Reece:Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Amgen: Consultancy, Honoraria, Research Funding; Takeda: Consultancy, Honoraria, Research Funding; Merck: Honoraria, Research Funding; Otsuka: Research Funding. Agarwal:Celgene Corporation: Employment, Equity Ownership. Chung:Celgene Corporation: Employment, Equity Ownership. Zafar:Celgene: Employment. Bahlis:Janssen: Consultancy, Honoraria, Research Funding; Celgene: Consultancy, Honoraria, Research Funding; Amgen: Consultancy, Honoraria, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal